
Billing operations for clinical practices and healthcare providers cover the administrative and technical steps that translate clinical encounters into claim transactions and payments. These processes typically include reviewing clinical documentation, assigning procedure and diagnosis codes, preparing and submitting claims to payers, posting payments, and maintaining records for compliance. In a United States context, these activities also interact with federal programs such as Medicare and Medicaid, and they must align with privacy and billing regulations that apply to covered entities.
Operationally, the workflow often begins with eligibility checks and ends with reconciliation of accounts receivable. Coding accuracy, timely submission, and follow-up on outstanding claims are recurring priorities because they influence cash flow and reporting. Staff roles may include front-desk eligibility verification, clinical coders, billing specialists, and managers who oversee payment posting and denials. Technology commonly used in these workflows includes practice management systems, electronic health record (EHR) modules, and clearinghouse services that exchange claims with payers.

Accurate clinical coding is central to these processes and typically relies on standardized systems used in the United States, such as ICD-10-CM for diagnoses and CPT/HCPCS for procedures. Documentation from clinicians must support code selection so claims reflect the services rendered; payers often audit or request medical records to verify coding. Coding workflows may include coder review, physician queries for clarification, and regular internal audits to detect patterns of denial or undercoding. Adherence to coding guidelines may reduce administrative friction but does not eliminate the need for follow-up.
Claim transmission commonly uses electronic data interchange (EDI) through clearinghouses or payer portals. Clearinghouses can validate file formats, check for common errors, and route claims to the appropriate payer, which may shorten processing times compared with manual submission. Remittance advice and electronic remittance advice (ERA) formats provide payment details that billing staff use to post payments and reconcile accounts. Practices often configure their EHR or billing software to accept ERAs and support automated posting where feasible, while retaining manual review for exceptions.
Denial management and appeals form a continuous feedback loop within billing operations. Denials may arise from eligibility issues, coding mismatches, missing documentation, or payer-specific rules. Effective denial workflows often include categorization of denial reasons, priority assignment based on expected recoverable dollars, and documentation of appeal outcomes. In the United States, familiarity with payer policies and Medicare claims processing guidance may help staff craft appropriate appeals and prevent recurrent denials, though outcomes depend on payer review and supporting records.
Patient billing and financial communication are also part of operational processes. Statements, itemized bills, and explanations of benefits are typical documents used to convey balances to patients and to coordinate patient responsibility with insurance payments. Privacy rules under U.S. law require safeguards for protected health information during billing communications. Practices may maintain financial counseling or payment-plan policies for patients while ensuring documentation for audit trails and reconciliation.
Overall, these elements combine into a revenue cycle framework that links front-office registration, clinical documentation, coding, claims submission, payment posting, and follow-up. Each stage may involve specific software tools and staff roles that vary by practice size and payer mix in the United States. The next sections examine practical components and considerations in more detail.
Operational components typically include patient registration, eligibility verification, charge capture, coding, claims submission, payment posting, and follow-up. In the United States, eligibility checks often involve screening for Medicare, Medicaid, or commercial plan coverage and verifying prior authorization requirements where applicable. Charge capture may be performed within an EHR or via a separate practice management system, and errors at this stage commonly lead to downstream denials. Clinics often map specific staff duties across these functions to maintain throughput and manage accounts receivable days.
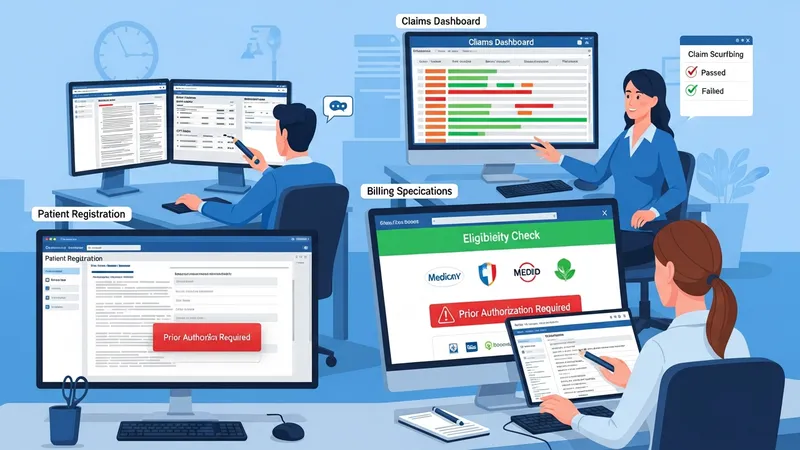
Staffing models vary across clinics: some maintain in-house teams for eligibility, coding, and follow-up; others outsource parts of the workflow to third-party RCM vendors or clearinghouses. Outsourced arrangements may aggregate volume across clients and provide specialized tools for claim scrubbing, while in-house teams retain direct control over documentation and patient interactions. When evaluating arrangements, clinics often consider interoperability with existing EHR systems, data security, and the ability to handle payer-specific requirements without compromising compliance with U.S. regulations.
Workflow automation can reduce manual data entry and repetitive checks. Examples of automation include electronic eligibility verification, automated claim scrubbing for format and common errors, and ERA-driven payment posting. Automation may shorten processing times and lower error rates in routine tasks, but practices typically retain manual review for complex claims, appeals, and clinical denials. Integration between clinical documentation and billing modules is a common operational priority in U.S. settings to ensure codes reflect clinical intent.
Operational monitoring often uses metrics such as clean claim rate, average days in accounts receivable, denial rate by reason, and collection percentage of billed charges. These indicators may help staff prioritize interventions; for instance, a spike in denials for missing prior authorizations may prompt process changes in registration. Practices in the United States may also benchmark performance against peer groups or published industry ranges, keeping in mind that payer mix and service lines materially influence typical values.
Coding in the United States typically relies on ICD-10-CM for diagnosis coding and CPT/HCPCS for reporting procedures and services. Accurate linkage between documentation and code selection is important for payer adjudication and for meeting medical necessity criteria used by Medicare and other payers. Clinics often implement coder review steps, physician query protocols for clarification, and periodic internal or external audits to detect misalignment between documentation and coded claims. Such audits may serve as compliance checks and help identify training needs for clinical or billing staff.

Compliance considerations extend beyond coding to include privacy, security, and billing regulations. U.S. providers must follow HIPAA privacy and security rules when transmitting billing information and when storing electronic claim files. Additionally, Medicare program rules and state Medicaid policies define coverage criteria, bundling rules, and documentation standards for claims. Regular review of payer policy updates and CMS guidance is a common compliance practice for clinics that bill federally funded programs.
Clinical documentation improvement (CDI) efforts may be used to clarify the medical record so coding accurately reflects the clinical picture. CDI programs often include education for clinicians about documentation elements that support code specificity, as well as retrospective reviews to identify documentation gaps. While improved documentation can reduce coding ambiguity and may reduce denials linked to insufficient information, clinics usually view CDI as part of broader quality and billing alignment rather than a guarantee of payment outcomes from any particular payer.
Audit readiness and response procedures are part of compliance planning. Clinics may maintain records of claims submissions, clinical notes, and correspondence with payers to support appeals or external reviews. When audits occur, documentation that corroborates the services billed is typically central to resolution. Many U.S. providers establish retention schedules and secure storage for billing records to meet both payer inquiries and regulatory obligations.
Claim submission in the United States commonly uses electronic formats (ANSI X12 EDI transactions) transmitted through clearinghouses or directly to payer portals. Clearinghouses perform validation checks for format, required fields, and common errors, which can reduce initial rejections. Electronic submission may accelerate initial processing compared with paper claims, though payer adjudication timelines still vary. Practices often configure their billing systems to generate claims in standard EDI formats and to receive electronic remittance advice (ERA) for automated payment posting.
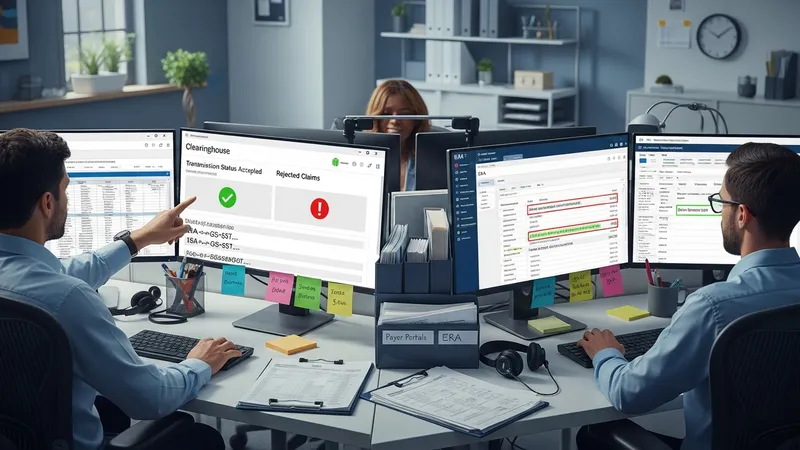
Clearinghouse services and payer connectivity choices influence routing, rejection handling, and reporting capabilities. Examples of U.S. clearinghouses include vendor platforms that support multiple payers and offer dashboard reporting for rejected claims and transmission statuses. When claims are rejected by a clearinghouse for formatting or data errors, billing staff typically correct and resubmit them. For accepted claims, remittance data received via ERA may be used to reconcile payments against billed charges and to identify underpayments or co-insurance amounts.
Payment posting procedures combine automated ERA posting with manual review for exceptions. Automated posting can match payment amounts and adjustments to claim lines, while denials and partial payments often require manual intervention to assign responsibility and plan appeals. Reconciliation practices may include daily matching of ERA to deposit batches and periodic review of payer payment patterns. Accurate posting supports downstream reporting on revenue, aging receivables, and cash flow projections for clinic management.
Data security and transaction logging are integral during submission and posting. Secure transmission protocols, access controls in billing systems, and audit logs help demonstrate compliance with privacy and security expectations in U.S. healthcare transactions. Practices often maintain vendor agreements that outline data handling responsibilities when external clearinghouses or RCM providers are part of the claim flow.
Denial management workflows often start with categorizing denials by reason code and estimating potential recoverable amounts. Common denial reasons in U.S. payers include eligibility discrepancies, coding errors, lack of medical necessity documentation, and prior authorization lapses. Practices may assign denials to specialized staff for appeals, correction and resubmission, or patient billing adjustments. Tracking denial trends can highlight systemic issues such as registration errors or documentation gaps that may be addressed through targeted process changes.

Patient billing and financial communication involve generating statements, applying insurance payments, and collecting patient-responsible balances in a transparent manner. Under U.S. privacy rules, clinics must safeguard patient information in billing exchanges. Patient financial discussions often include explanation of benefits (EOBs) interpretation, payment plan options, and documentation of communications. Practices that serve Medicare and Medicaid populations may also follow specific federal and state guidelines for patient liability and balance billing limitations.
Revenue reconciliation ties posted payments and adjustments back to deposited funds and payer remittances. Reconciliation procedures may include matching ERAs to deposits, investigating differences due to payer edits or contractual adjustments, and preparing reports for accounting staff. Timely reconciliation supports accurate financial records and can reveal issues such as recurring underpayments by a particular payer, which may warrant appeals or contract review.
Key performance indicators used to monitor revenue cycle health commonly include days in accounts receivable (A/R), clean claim rate, denial rate, and collection ratio. These metrics may be interpreted in the context of practice size, payer mix, and service lines. Ongoing measurement and periodic review of workflow steps allow clinics to identify bottlenecks, evaluate vendor performance when third-party services are used, and adjust internal controls to support reliable billing and reimbursement processes.