
Cancer treatment commonly involves a set of conventional medical approaches paired with supportive care services. Conventional modalities are interventions that target cancer cells directly or remove affected tissue; they include surgical procedures, radiation therapy, and systemic drug treatments. Supportive care encompasses symptom management, rehabilitation, nutritional guidance, psychosocial support, and palliative approaches that address quality-of-life concerns across the illness trajectory. Together, these components form integrated pathways intended to control disease manifestations, relieve symptoms, and help patients maintain function during and after active treatment.
Descriptions of these care elements emphasize roles rather than promises: surgical, radiation, and systemic therapies may reduce tumor burden or manage local effects, while supportive services may address pain, fatigue, emotional distress, and functional needs. Clinical teams typically assess disease characteristics, patient health status, and treatment goals to propose combinations of modalities. Coordination among specialists—surgeons, radiation oncologists, medical oncologists, palliative care clinicians, nursing staff, and allied professionals—often shapes how conventional modalities and supportive care are sequenced and adjusted over time.

Comparative framing between modalities often focuses on mechanism and scope: surgery and radiation are primarily local or regional approaches, while systemic therapies act throughout the body. Each modality may be chosen alone or combined based on tumor type, stage, and patient factors; combinations may aim to improve local control, reduce recurrence risk, or palliate symptoms. Clinical decision frameworks commonly articulate intended outcomes (for example, curative, adjuvant, neoadjuvant, or palliative aims) rather than absolute expectations. These frameworks may guide sequencing and supportive-service involvement during treatment phases.
Supportive care commonly includes symptom assessment and management, which may address pain, nausea, fatigue, and functional impairments that arise from both disease and its treatments. Multidisciplinary teams can include pain specialists, physiotherapists, dietitians, social workers, and mental health clinicians. Early involvement of supportive services often aims to maintain function and daily activity levels, and to address psychosocial stressors. Evidence summaries and clinical guidelines often suggest that timely supportive interventions may reduce symptom burden and improve care coordination, recognizing outcomes can vary by individual circumstances.
Integration of modalities typically requires coordination across specialties and settings. Tumor boards or multidisciplinary case reviews may bring specialists together to align on staging, treatment sequencing, and anticipated supportive needs. Treatment plans often include monitoring schedules, imaging intervals, and criteria for modifying therapy if toxicity or progression occurs. Patient preferences and goals of care are commonly discussed within this planning context to ensure that modality selection and supportive resources reflect individual priorities and medical realities.
Risk management and toxicity mitigation are central considerations when combining conventional treatments. Each modality carries potential adverse effects—surgical complications, radiation-induced tissue changes, or systemic treatment toxicities—which supportive care aims to anticipate and manage. Prehabilitation and rehabilitation services may be used to optimize fitness before surgery and to restore function afterward. Clinical teams often apply standard assessment tools to monitor toxicity and adjust supportive measures; such tools can guide interventions without implying uniform outcomes for every person.
In summary, conventional cancer modalities and supportive care represent complementary components of comprehensive oncology practice. Modalities typically target disease control at local or systemic levels, while supportive services address symptoms, function, and psychosocial needs. Effective integration often involves multidisciplinary coordination, planned monitoring, and tailored supportive interventions that respond to evolving clinical status. The next sections examine practical components and considerations in more detail.
Surgical approaches are commonly used to remove primary tumors or to obtain diagnostic tissue. Procedures vary from minimally invasive resections to more extensive operations and may include lymph node sampling or reconstruction. When surgery is planned, supportive care considerations can include preoperative assessment, optimization of nutrition and comorbid conditions, and postoperative rehabilitation. Teams often evaluate risk factors for complications and may recommend physical therapy or wound care support after surgery. Discussions about expected recovery timelines and potential functional impacts typically occur as part of shared planning without prescriptive guarantees.

Local control strategies often interact with other modalities: surgery may be followed by radiation or systemic therapy to lower recurrence risk in certain contexts. Timing and sequencing depend on tumor biology, margins, staging, and patient fitness. For example, neoadjuvant (pre-surgery) systemic therapy may be used to reduce tumor size, while adjuvant (post-surgery) treatments may address microscopic disease. Supportive care during these intervals commonly focuses on perioperative symptom management, mobility preservation, and psychosocial support to aid recovery and adherence to subsequent therapy.
Risk reduction and rehabilitation are integral to surgical care pathways. Prehabilitation programs may include exercise, nutritional counseling, and smoking cessation support that can often improve baseline fitness before major procedures. Postoperative rehabilitation may address mobility, range of motion, and activities of daily living. Pain control strategies and monitoring for surgical complications typically involve nursing and specialty consults. These supportive elements aim to improve short-term recovery metrics and facilitate timely access to any planned adjuvant treatments.
Coordination between surgical teams and supportive services can improve continuity of care. Multidisciplinary care plans may outline expected follow-up intervals, criteria for wound checks, and indicators for escalation of symptoms. Clear communication among surgeons, medical teams, primary care providers, and allied professionals often helps manage transitions from inpatient to outpatient settings. Such coordination is presented as a common organizational approach and not as a guarantee of specific outcomes for individual patients.
Radiation therapy uses targeted ionizing radiation to treat localized disease and may be delivered as external beam radiation, stereotactic techniques, or brachytherapy. Planning relies on imaging and dosimetric calculations to balance tumor control with preservation of surrounding tissue. Supportive care considerations with radiation often include skin care guidance, management of fatigue, and monitoring for organ-specific effects that can emerge during or after treatment. Multidisciplinary input from radiation oncologists, nurses, and supportive clinicians typically informs symptom surveillance strategies.
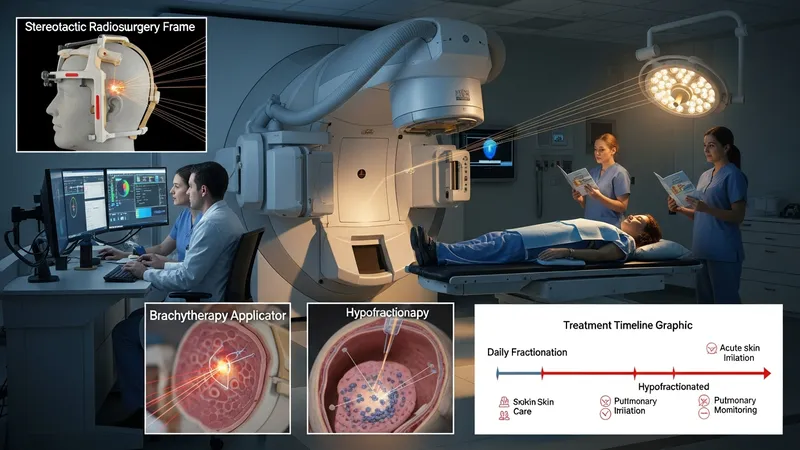
Fractionation schedules and delivery techniques vary by indication: some regimens involve daily treatments for several weeks, while others use higher-dose, fewer-fraction approaches. Each approach has different patterns of acute and late effects; for example, shorter high-dose regimens may have distinct toxicity profiles compared with conventional fractionation. Supportive services are often tailored to the anticipated side-effect timeline and may include dietary modifications, swallowing therapy for head and neck radiotherapy, or pulmonary monitoring for thoracic treatments.
Proactive symptom management is frequently emphasized in radiation care pathways. Clinicians may use validated assessment tools to track fatigue, mucositis, dermatitis, or other site-specific reactions and to guide interventions such as analgesia, topical care, and rehabilitative therapies. Coordination with systemic therapy schedules is important when radiation is combined with systemic agents, as combined modalities can influence toxicity risk. Planning conversations commonly consider the cumulative impact of modalities and the supportive measures needed to maintain function.
Follow-up after radiation often includes surveillance imaging and clinical assessments to evaluate response and late effects. Supportive care may extend into survivorship, addressing chronic symptoms or functional limitations that persist. Rehabilitation services and psychosocial support can assist with long-term quality-of-life concerns. These care elements are typically structured as options within multidisciplinary survivorship planning rather than definitive outcomes applicable to every individual.
Systemic therapies encompass a broad range of drugs that circulate through the body to affect cancer cells, including cytotoxic chemotherapy, hormonal agents, targeted therapies directed at molecular features, and immune-modulating treatments. Each class typically has distinct mechanisms, administration schedules, and toxicity profiles. Supportive care in this context frequently includes management for nausea, infection risk, blood count changes, and other organ-specific effects. Pharmacists, infusion nurses, and specialist clinicians often collaborate to monitor and manage these issues throughout treatment cycles.

Administration settings can include outpatient infusion centers, oral therapy at home, or inpatient care for complex needs. Adherence considerations differ by route: orally administered agents may require patient education on dosing schedules and interactions, while infusion treatments involve on-site monitoring for immediate reactions. Supportive services such as medication counseling, coordination with primary care, and home-based symptom check-ins are commonly used to address practical aspects of systemic therapy, recognizing that individual needs and responses vary.
Managing toxicities from systemic agents often involves routine laboratory monitoring and dose adjustments guided by standardized protocols. Growth factor support, antiemetics, and antimicrobial prophylaxis are examples of measures that may be used to reduce specific risks. Palliative and supportive care providers can work alongside oncology teams to address complex symptom clusters, polypharmacy considerations, and functional decline. These collaborative approaches are presented as common frameworks rather than guarantees applicable in every case.
Integration across systemic and local modalities often requires careful scheduling to balance efficacy and safety. For instance, the timing of chemotherapy relative to surgery or radiation may be planned to optimize outcomes while limiting overlapping toxicities. Multidisciplinary discussions and clear communication about monitoring plans can help align expectations and supportive resources. Such coordination is described as a routine element of comprehensive care planning rather than an assurance of a particular trajectory for any patient.
Supportive care covers a spectrum of services designed to manage symptoms, maintain function, and address psychosocial needs during and after cancer-directed treatments. Common components include pain and symptom management, nutritional support, physical and occupational therapy, mental health services, and spiritual or social support. These services may be provided concurrently with curative-intent therapies or as part of palliative-focused care, depending on individual goals and clinical context. The intent is to reduce symptom burden and improve functional outcomes where possible, recognizing variability in individual responses.

Care coordination mechanisms—such as multidisciplinary clinics, nurse navigators, or case conferences—are frequently used to organize services across specialties and settings. Effective coordination may include shared care plans, scheduled follow-up assessments, and clear communication channels among providers and patients. Evidence summaries often note that coordinated supportive services can enhance access to symptom management and reduce fragmentation of care, although specific models and outcomes may differ by institution and healthcare system.
Psychosocial and practical supports commonly address emotional distress, caregiver burden, and logistical challenges related to treatment schedules. Counseling, peer-support groups, and social work assistance for transportation or financial counseling are examples of services that may be available. Rehabilitation and survivorship programs often focus on restoring activity levels, vocational concerns, and long-term symptom monitoring. These elements are described as typical components of comprehensive supportive care pathways, presented without prescriptive language about outcomes.
Ongoing assessment and individualized planning are central to supportive care. Validated screening tools for distress, symptom scales, and functional assessments can guide referrals and interventions. Teams may periodically reassess goals of care and adapt supportive measures as treatment phases change. Readers should understand these structures as common practice frameworks used to align conventional modalities with supportive services, with the aim of optimizing care processes rather than promising specific results.